


– there is no pandemic
Part II
Global Research, December 10, 2021
Theme: Science and Medicine
All Global Research articles can be read in 51 languages by activating the “Translate Website” drop down menu on the top banner of our home page (Desktop version).
Visit and follow us on Instagram at @crg_globalresearch.
***
First published on November 23, 2021
“The PCR is a Process. It does not tell you that you are sick”.
Dr. Kary Mullis, Nobel Laureate and Inventor of the RT-PCR, passed away in August 2019.
“…All or a substantial part of these positives could be due to what’s called false positives tests.”
Dr. Michael Yeadon: former Vice President and Chief Science Officer for Pfizer
This misuse of the RT-PCR technique is applied as a relentless and intentional strategy by some governments to justify excessive measures such as the violation of a large number of constitutional rights, … under the pretext of a pandemic based on a number of positive RT-PCR tests, and not on a real number of patients.
.Dr. Pascal Sacré, Belgian physician specialized in critical care and renowned public health analyst.
To read PART I of this article click link below
The Covid-19 Pandemic Does Not Exist
By Prof Michel Chossudovsky, November 15, 2021
***
Introduction
Media lies coupled with a systemic and carefully engineered fear campaign have sustained the image of a killer virus which is relentlessly spreading to all major regions of the World.
Several billion people in more than 190 countries have been tested (as well as retested) for Covid-19.
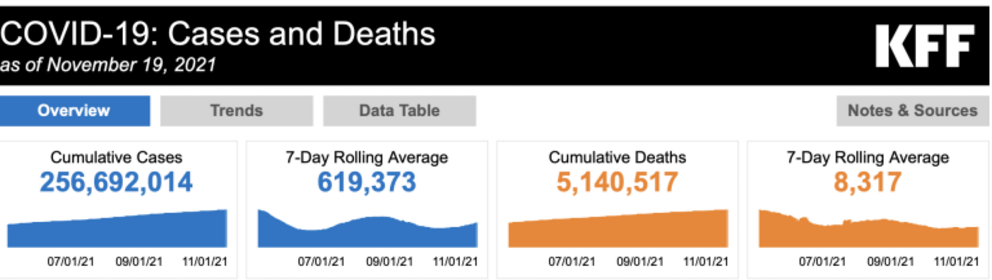
At the time of writing, approximately 260 million people Worldwide have been categorized as “confirmed Covid-19 cases”. The alleged pandemic is said to have resulted in more than 5 million Covid-19 related deaths.
Both sets of figures: morbidity and mortality are invalid. A highly organized Covid testing apparatus (part of which is funded by the billionaire foundations) has been established with a view to driving up the numbers of “Confirmed Covid-19 Cases”, which are then used as a justification to impose the “vaccine” passport coupled with the repeal of fundamental human rights.

A so-called “Global Tracker System” has been established with an interactive map pointing to global as well as country level trends and weekly tendencies.
A Fourth Wave has been announced. Invalid figures pertaining to Covid-19 are routinely plastered on the news tabloids.

Meanwhile, both the media and the governments have turned a blind eye to the rising trend of Covid-19 vaccine deaths and adverse events, which are confirmed by “official” government agencies. (See below)
TOTAL for EU/UK/USA
45,250 Covid-19 injection related deaths, 7,418,980 injuries
EudraVigilance Database, MHRA Yellow Card Scheme. VAERS database.
The Reverse Transcription Polymerase Chain Reaction Test (RT-PCR)
The slanted methodology applied under WHO guidance for detecting the alleged spread of the virus is the Polymerase Chain Reaction Test (RT-PCR), which is routinely applied all over the World.
The RT-PCR Test has been used Worldwide to generate millions of erroneous “Confirmed Covid-19 cases”, which are then used to sustain the illusion that the alleged pandemic is Real.
This assessment based on erroneous numbers has been used in the course of the last 20 months to spearhead and sustain the fear campaign.
And people are now led to believe that the Covid-19 “vaccine” is the “solution”. And that “normality” will be restored once the entire population of Planet Earth has been vaccinated.
“Confirmed” is a misnomer: A “Confirmed RT-PCR Positive Case” does not Imply a “Confirmed Covid-19 Case”.
Positive RT-PCR is not synonymous with COVID-19 disease! PCR specialists make it clear that a test must always be compared with the clinical record of the patient being tested, with the patient’s state of health to confirm its value [reliability] (Dr. Pascal Sacré)
The procedure used by the national health authorities is to categorize all RT-PCR positive cases, as “Confirmed Covid-19 Cases” (with or without a medical diagnosis). Ironically, this routine process of identifying “confirmed cases” . is in derogation of the CDC’s own guidelines:
“Detection of viral RNA may not indicate the presence of infectious virus or that 2019-nCoV is the causative agent for clinical symptoms. The performance of this test has not been established for monitoring treatment of 2019-nCoV infection. This test cannot rule out diseases caused by other bacterial or viral pathogens.” (emphasis added)
In this article we will present detailed evidence that the methodology used to detect and estimate the spread of the virus is flawed and invalid.
1. False Positives
The earlier debate at the outset of the crisis focused on the issue of “False Positives”.
Acknowledged by the WHO and the CDC, the RT-PCR Test was known to produce a high percentage of false positives. According to Dr. Pascal Sacré:
“Today, as authorities test more people, there are bound to be more positive RT-PCR tests. This does not mean that COVID-19 is coming back, or that the epidemic is moving in waves. There are more people being tested, that’s all.”
The debate on false positives (acknowledged by the health authorities) points to so-called errors without necessarily questioning the overall validity of the RT-PCR test as a means to detecting the alleged spread of the CoV-SARS-2 virus.
2. The PCR-Test Does Not Detect the Identity of the Virus
The RT-PCR test does not identify/ detect the virus. What the PCR test identifies are genetic fragments of numerous viruses (including influenza viruses types A and B, and coronaviruses which trigger common colds).
The results of the TR-PCR test cannot “confirm” whether an individual who undertakes the test is infected with Covid-19.
According to Dr. Kary Mullis, inventor of the PCR technique: “The PCR detects a very small segment of the nucleic acid which is part of a virus itself.”According to renowned Swiss immunologist Dr B. Stadler
So if we do a PCR corona test on an immune person, it is not a virus that is detected, but a small shattered part of the viral genome. The test comes back positive for as long as there are tiny shattered parts of the virus left. Even if the infectious viri are long dead, a corona test can come back positive, because the PCR method multiplies even a tiny fraction of the viral genetic material enough [to be detected].
Dr. Pascal Sacré concurs: “These tests detect viral particles, genetic sequences, not the whole virus.”
In an attempt to quantify the viral load, these sequences are then amplified several times through numerous complex steps that are subject to errors, sterility errors and contamination.
3. The WHO’s “Customized” RT-PCR Covid-19 “Test”
Two important and related issues.
The PCR Test does not identify the virus as outlined above. Moreover, the WHO in January 2020, did not possess an isolate and purified sample of the novel 2019-nCov virus.
What was contemplated in January 2020 was a “customization”of the PCR test by the WHO, under the scientific guidance of the Berlin Virology Institute at Charité Hospital.
Dr. Christian Drosten, and his colleagues of the Berlin Virology Institute undertook a study entitled, “Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR”.
The title of the Berlin Virology Institute Study is an obvious misnomer. The PCR test cannot “detect” the 2019 novel coronavirus. (See Dr. Kary Mullis, Dr. B. Stadler, Dr. Pascal Sacré quoted in Section 2).
Moreover, the study, published by Eurosurveillance acknowledges that the WHO did not possess an isolate and purified sample of the novel 2019-nCov virus:
[While]… several viral genome sequences had been released,… virus isolates or samples [of 2019-nCoV] from infected patients were not available …”The Drosten et al team then recommended to the WHO, that in the absence of an isolate of the 2019-nCoV virus, a similar 2003-SARS-CoV should be used as a “proxy” of the novel virus:
“The genome sequences suggest presence of a virus closely related to the members of a viral species termed severe acute respiratory syndrome (SARS)-related CoV, a species defined by the agent of the 2002/03 outbreak of SARS in humans [3,4].
We report on the the establishment and validation of a diagnostic workflow for 2019-nCoV screening and specific confirmation [using the RT-PCR test], designed in absence of available virus isolates or original patient specimens. Design and validation were enabled by the close genetic relatedness to the 2003 SARS-CoV, and aided by the use of synthetic nucleic acid technology.” (Eurosurveillance, January 23, 2020, emphasis added).
What this ambiguous statement suggests is that the identity of 2019-nCoV was not required and that “Confirmed Covid-19 Cases” (aka infection resulting from the novel 2019 coronavirus) would be validated by “the close genetic relatedness to the 2003-SARS-CoV.”
What this means is that a coronavirus detected 19 years ago (2003-SARS-CoV) is being used to “validate” the identity of a so-called “novel coronavirus” first detected in China’s Hubei Province in late December 2019.
The recommendations of the Drosten study (generously supported and financed by the Gates Foundation) were then transmitted to the WHO. They were subsequently endorsed by the Director General of the WHO, Tedros Adhanom.
The WHO did not have in its possession the “virus isolate” required to identify the virus. It was decided that an isolate of the new coronavirus was not required.
The Drosten et al article pertaining to the use of the RT-PCR test Worldwide (under WHO guidance) was challenged in a November 27, 2020 study by a group of 23 international virologists, microbiologists et al.
It stands to reason that if the PCR test uses the 2003 SARS- CoV virus as “a point of reference”, there can be no “confirmed” Covid-19 cases resulting from the novel virus 2019-nCoV, subsequently renamed SARS-CoV-2.
4. Has the Identity of the 2019-nCoV Been Confirmed? Does the Virus Exist?
While the WHO did not possess an isolate of the virus, is there valid and reliable evidence that the 2019 novel coronavirus had been isolated from an “unadulterated sample taken from a diseased patient”?
The Chinese authorities announced on January 7, 2020 that “a new type of virus” had been “identified” “similar to the one associated with SARS and MERS” (related report, not original Chinese government source). The underlying method adopted by the Chinese research team is described below:
We prospectively collected and analysed data on patients with laboratory-confirmed 2019-nCoV infection by real-time RT-PCR and next-generation sequencing.
Data were obtained with standardised data collection forms shared by WHO and the International Severe Acute Respiratory and Emerging Infection Consortium from electronic medical records. (emphasis added)
The above study (quotation above as well as other documents consulted ) suggest that China’s health authorities did not undertake an isolation / purification of a patient’s specimen.
Using “laboratory-confirmed 2019-nCoV infection by real-time RT-PCR” is an obvious misnomer, i.e. the RT-PCR test cannot under any circumstances be used to identify the virus. (see section 2 above). The isolate of the virus by the Chinese authorities is unconfirmed.
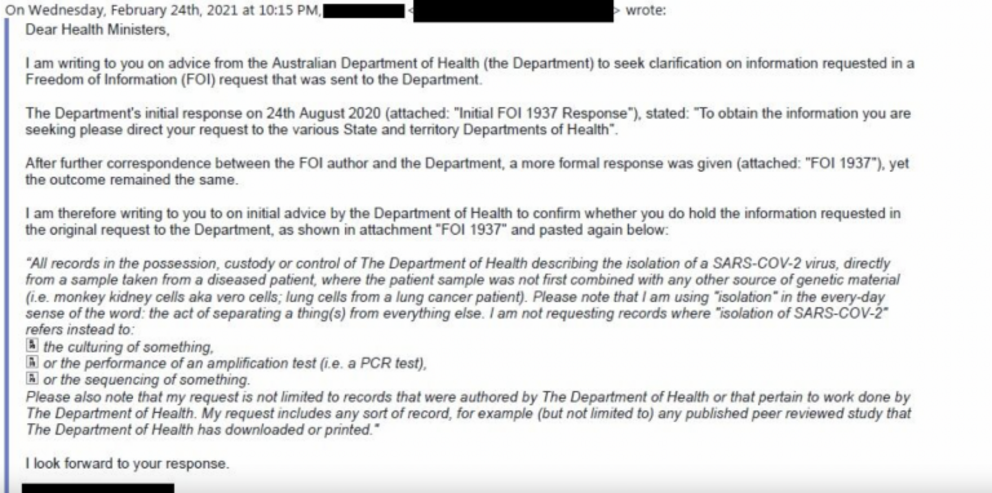
Freedom of Information Pertaining to the Isolate of SARS-CoV-2
A detailed investigative project by Christine Massey, entitled: Freedom of Information Requests: Health/ Science Institutions Worldwide “Have No Record” of SARS-COV-2 Isolation/Purification provides documentation concerning the identity of the virus.
Freedom of Information (FOI) requests were addressed to ninety Health /Science institutions in a large number of countries.
The responses to these requests confirm that there is no record of isolation / purification of SARS-CoV-2 “having been performed by anyone, anywhere, ever.”
“The 90 Health /Science institutions that have responded thus far have provided and/or cited, in total, zero such records:
Our requests [under “freedom of information”] have not been limited to records of isolation performed by the respective institution, or limited to records authored by the respective institution, rather they were open to any records describing “COVID-19 virus” (aka “SARS-COV-2”) isolation/purification performed by anyone, ever, anywhere on the planet.”
See also: 90 Health/Science Institutions Globally All Failed to Cite Even 1 Record of “SARS-COV-2” Purification, by Anyone, Anywhere, Ever, By Fluoride Free Peel, August 04, 2021
5. The Threshold Amplification Cycles. The WHO Admits that the The Results of the RT-PCR “Test” are Totally Invalid
The rRT-PCR test was adopted by the WHO on January 23, 2020 as a means to detecting the SARS-COV-2 virus, following the recommendations of the Berlin Virology research group (quoted above).
Exactly one year later on January 20th, 2021, the WHO retracts. They don’t say “We Made a Mistake”. The retraction is carefully formulated. (See original WHO document here)
Below are selected excerpts from my article entitled: The WHO Confirms that the Covid-19 PCR Test is Flawed: Estimates of “Positive Cases” are Meaningless. The Lockdown Has No Scientific Basis
The contentious issue pertains to the number of amplification threshold cycles (Ct). According to Pieter Borger, et al
The number of amplification cycles [should be] less than 35; preferably 25-30 cycles. In case of virus detection, >35 cycles only detects signals which do not correlate with infectious virus as determined by isolation in cell culture…(Critique of Drosten Study)
The World Health Organization (WHO) tacitly admits one year later that ALL PCR tests conducted at a 35 cycle amplification threshold (Ct) or higher are INVALID. But that is what they recommended in January 2020, in consultation with the virology team at Charité Hospital in Berlin.
If the test is conducted at a 35 Ct threshold or above (which was recommended by the WHO), genetic segments of the SARS-CoV-2 virus cannot be detected, which means that ALL the so-called “Confirmed Covid-19 Cases” tabulated Worldwide in the course of the last 22 months are invalid.
According to Pieter Borger, Bobby Rajesh Malhotra, Michael Yeadon, et al, the Ct > 35 has been the norm “in most laboratories in Europe & the US”.
The WHO’s Mea Culpa
Below is the WHO’s carefully formulated “Retraction”.
“WHO guidance Diagnostic testing for SARS-CoV-2 states that careful interpretation of weak positive results is needed (1). The cycle threshold (Ct) needed to detect virus is inversely proportional to the patient’s viral load. Where test results do not correspond with the clinical presentation, a new specimen should be taken and retested using the same or different NAT technology. (emphasis added)
WHO reminds IVD users that disease prevalence alters the predictive value of test results; as disease prevalence decreases, the risk of false positive increases (2). This means that the probability that a person who has a positive result (SARS-CoV-2 detected) is truly infected with SARS-CoV-2 decreases as prevalence decreases, irrespective of the claimed specificity.”
“Invalid Positives” is the Underlying Concept
This is not an issue of “Weak Positives” and “Risk of False Positive Increases”. What is at stake is a “Flawed Methodology” which leads to invalid estimates of “Confirmed Covid-19 Cases”.
What this admission of the WHO confirms is that the estimate of covid positive from a PCR test (with an amplification threshold of 35 cycles or higher) is invalid. In which case, the WHO recommends retesting: “a new specimen should be taken and retested…”.
The WHO calls for “Retesting”, which is tantamount to saying “We Screwed Up”.
That recommendation is pro-forma. It won’t happen. Several billion people Worldwide have already been tested, starting in early February 2020. Nonetheless, we must conclude that unless retested, those estimates (according to the WHO) are invalid.
From the outset, the PCR test has routinely been applied at a Ct amplification threshold of 35 or higher, following the January 2020 recommendations of the WHO. What this means is that the PCR methodology as applied Worldwide has in the course of the last 20 months led to the compilation of faulty and misleading Covid statistics.
And these are the statistics which are used to measure the progression of the so-called “pandemic”. Above an amplification cycle of 35 or higher, the test will not detect fragments of the virus. Therefore, the official “covid numbers” (Confirmed Covid-19 Cases) are meaningless.
It follows that there is no scientific basis for confirming the existence of a pandemic.
Which in turn means that the lockdown / economic measures which have resulted in social panic, mass poverty and unemployment (allegedly to curtail the spread of the virus) have no justification whatsoever.
According to scientific opinion:
“if someone is tested by PCR as positive when a threshold of 35 cycles or higher is used (as is the case in most laboratories in Europe & the US), the probability that said person is actually infected is less than 3%, the probability that said result is a false positive is 97% (Pieter Borger, Bobby Rajesh Malhotra, Michael Yeadon, Clare Craig, Kevin McKernan, et al, Critique of Drosten Study)
As outlined above, “the probability that said result is a false positive is 97%”: It follows that using the >35 cycles detection will indelibly contribute to “hiking up” the number of “fake positives”.
The WHO’ Mea Culpa confirms that the Covid-19 PCR test procedure as applied is invalid.
Was the 2009 H1N1 Pandemic a “Dress Rehearsal”?
In 2009 a H1N1 pandemic allegedly affecting 2 billion people was carried out by the WHO.
Corruption at the highest levels of the WHO: Several critics including Dr. Wolfgang Wodarg confirmed that the H1N1 Pandemic was “Fake”
The Parliamentary Assembly of the Council of Europe (PACE), a human rights watchdog, is publicly investigating the WHO’s motives in declaring a pandemic. Indeed, the chairman of its influential health committee, epidemiologist Wolfgang Wodarg, has declared that the “false pandemic” is “one of the greatest medicine scandals of the century.” (Michael Fomento, Forbes, February 10, 2010)
In retrospect, the COVID-19 “pandemic” is far more serious and diabolical than the 2009 H1N1.
See Dr. Wolfgang Wodarg incisive and carefully documented analysis of the RT-PCR test as applied by the WHO in relation to Covid-19.

Concluding Remarks
The RT-PCR Test is the Smoking Gun. It invalidates Everything.
There is no such thing as a “Confirmed Covid-19 Case”. The entire data bank is invalid.
At the time of writing, the number of tabulated so-called “Confirmed Covid-19 Cases” is of the order of 260 million Worldwide. These numbers are totally meaningless.
None of this data can be categorized as “Confirmed”.
The PCR Test does not identify the novel virus, and the genetic fragments of a so-called “similar” 2003 coronavirus (SARS-1) cannot be used as a means to identify the virus which causes Covid-19, nor can it be used to identify the deadly variants of the 2019 novel coronavirus.
Moreover, according to the Freedom of Information (FOI) study quoted above, the isolate of the novel coronavirus is unconfirmed.
Sustained by a complexity of lies, the covid-19 narrative is extremely fragile. This consensus relies on fake science and a totally invalid data bank of alleged “confirmed Covid-19 cases”.
There is no pandemic.
And in the absence of a Covid-19 pandemic, there is no scientific justification for implementing the Covid-19 “Vaccine” which has resulted in a Worldwide trend of deaths and injuries:
How did Big Pharma manage to develop a vaccine (sponsored by the WHO, GAVI, the Gates Foundation, et al) with a mandate “to protect people” against a virus which has not been isolated/ purified from an “unadulterated sample taken from a diseased patient”?
Vaccine in relation to What? The virus has not been identified.
Moreover, 2019 SARS-CoV-2 has been categorized as similar to the 2003 SARS-CoV which means that the 2019 SARS-CoV-2 is not a novel virus.
The legitimacy of the Covid vaccine project hinges upon the validity of hundreds of thousands of RT-PCR fake positive cases Worldwide combined with fake Covid related mortality data. ( See Michel Chossudovsky, Does the Virus Exist)
What lies ahead?
National governments have announced a Fifth Wave, focussing on the alleged “deadly variants” of SARS-CoV-2, including the Delta variant.
The variant is a scam. How do they identify the “variants”. The PCR test neither detects the virus nor the variants of the virus.
There is no isolate of the novel coronavirus on record. Moreover, the WHO’s “customized” PCR test uses as a proxy a similar 2003 SARS-CoV virus (which no doubt has mutated extensively over the last 19 years).
“Restrictions would have to be reintroduced”. … the Delta variant poses a “higher risk of hospitalisations”
These announcements are intended to justify a continuation of repressive policy measures, the speeding up of the vaccination program, as well as the repression of the protest movement.
There is no Pandemic. The Endgame is Tyranny.
The Pandemic is being used to Impose a New World Order.
When the Lie Becomes the Truth, There is No Moving Backwards.
The first Step is to Dismantle the Propaganda Apparatus.
The Elite’s Covid Consensus is Extremely Fragile.
There is no Pandemic. They Do not have a Leg to Stand on.
That Consensus must be broken.
***
See Michel Chossudovsky’s E-Book (13 Chapters) entitled
See also
Does the Virus Exist? SARS-CoV-2 Has Not Been Isolated? “Biggest Fraud in Medical History”
See Michel Chossudovsky, Biographical Note
Michel Chossudovsky’s Articles on Global Research
The original source of this article is Global Research
Copyright © Prof Michel Chossudovsky, Global Research, 2021