

Fake News?
The prevailing corona nonsense narrative
Dec
I studied medicine at the University of Zurich, obtained a doctorate in immunology and virology, specialized in internal medicine and cardiology and have 33 years of experience in diagnosis and therapy of acute respiratory infections, in hospitals, in intensive care units and, for 23 years, in my medical practice.
In February 2020, I sat in my practice and was amazed. What I had learned in medical school, during my scientific training and in my practical medical work was suddenly turned upside down. Anyone who felt even a sore throat, no longer treated himself, to visit his or her GP only if the symptoms got worse, but ran to the nearest hospital with the request to be tested immediately, and with the fear of perhaps having to die, and not only having to die, but perhaps of having to suffocate miserably.
Worldwide, the prevailing corona narrative was established in a very short period. At the same time, humanity was divided into its supporters and opponents. Such an extent of division of the society we have never experienced before. It divides friendships, families, and even partnerships. Such a division is always an expression of the fact that a large part of humanity is not living in reality, but is caught up in a context of delusion imposed by a handful of psychopaths and their many narcissistic lackeys. In such a situation, we must always ask ourselves first: “Am I a realist, or in fact a totally deluded one?” This question can only be answered by looking at reality as soberly as possible.
It is my duty as a doctor to treat my patients to the best of my knowledge. This includes to inform them about their disease in a way that laypeople can understand and make informed decisions about what to do.
In February / March 2020 I realised that it is my duty as a doctor to educate the public about this disease of the whole society, in a way that laypeople can understand and make informed decisions about what to do. I am still doing this, no more but also no less, and nobody and nothing will stop me from continuing to do so.
I confront the myths and intellectual absurdities of the prevailing corona narrative with the scientific evidence. I do this chronologically, and so that also laypeople can understand and make informed decisions as to what further actions seem appropriate, for themselves and for their loved ones.
Scientific references to my statements can be found on the homepages of ‘Aletheia – our Swiss network of doctors and scientists for proportionality’, of the ‘Corman-Drosten Review Report’, and of ‘Doctors for Covid Ethics’, all of which I am a member, and on my simple homepage, which I had created after having been banned from social media.
PCR Testing Epidemic, 2006
As responsible physicians and scientists, in the case of infections diagnosed by quick PCR tests, especially in the context of an alleged epidemic of national or pandemic of international scope, we must always consider the possibility of a pseudo or testing epidemic.
In 2007, the New York Times, virtually the bible of journalists whose integrity they still trusted at the time, publishes an important piece entitled: ‘Faith in Quick Test Leads to Epidemic That Wasn’t’.
Dr. Herndon, internist at a medical centre in the U.S. state of New Hampshire, coughs seemingly incessantly for a fortnight starting in mid-April 2006. Soon, an infectious disease specialist has the disturbing idea that this could be the beginning of a pertussis epidemic. By the end of April, other hospital staff are also coughing. Severe, persistent coughing is a leading symptom of whooping cough. And if it is whooping cough, the outbreak must be contained immediately because the disease can be fatal for babies in the hospital and lead to dangerous pneumonia in frail elderly patients.
It is the start of a bizarre episode: the story of an epidemic that wasn’t.
For months, almost everyone involved believes there is a huge whooping cough outbreak at the medical centre with far-reaching consequences. Nearly 1,000 staff members are given a quick PCR test and put on leave from work until the results are in; 142 people, 14.2% of those tested, including Dr. Herndon, are positive on the quick PCR test and diagnosed with pertussis. Thousands, including many children, receive antibiotics and a vaccine as protection. Hospital beds are taken out of service as a precaution, including some in the intensive care unit.
Months later, all those apparently suffering from whooping cough are stunned to learn that bacterial cultures, the diagnostic gold standard for pertussis, could not detect the bacterium that causes whooping cough in any single sample. The whole insanity was a false alarm.
The supposed pertussis epidemic had not taken place in reality, but only in the minds of those involved, triggered by blind faith in a highly sensitive quick PCR test that had become, oh, so modern. In truth, all those who had fallen ill had suffered from a harmless cold. Infectiologists and epidemiologists had put aside their expertise and common sense and blatantly ignored this most likely differential diagnosis of the symptom cough.
Many of the new molecular tests are quick but technically demanding. Each laboratory performs them in its own way as so-called ‘home brews’. Often they are not commercially available and there are rarely good estimates of their error rates. Their high sensitivity makes false positives likely. When hundreds or thousands of people are tested, as happened here, false-positive results can give the appearance of an epidemic.
An infectiologist said, I had a feeling at the time that this gave us a shadow of a hint of what it might be like during a pandemic flu epidemic.
And an epidemiologist explained: One of the most troubling aspects of the pseudo-epidemic is that all the decisions seemed so sensible at the time.
The madness of a pseudo or testing epidemic had seemed perfectly normal to so many people involved.
I recommend you read this article published in the New York Times in 2007 and ask yourself: “Shouldn’t we all have learned a lot from this for the future?”
Swine Flu Scandal, 2009
As responsible physicians and scientists, in an alleged or real epidemic of national or pandemic of international scope we must always remember previous alleged or real epidemics and pandemics. Here is the last allegedly serious pandemic: The swine flu scandal.
In spring 2009, a highly contagious, very dangerous influenza virus, H1N1, seems to threaten humanity. The disease it causes is clinically indistinguishable from seasonal flu. It is called swine flu.
Experts like the German virologist Prof. Christian Drosten spread horror scenarios predicting millions of deaths worldwide. In May, the WHO relaxes the criteria for declaring a pandemic for reasons that have never been explained. It removes the dangerousness of the causative pathogen from the definition of a pandemic. Now, the rapid massive spread of a comparatively harmless pathogen over at least two WHO regions is enough. Any endemic, every seasonal wave of any flu or cold virus, no matter how harmless it is, can be called a pandemic. Promptly, the WHO declares an H1N1 pandemic on June 11th.
Politicians are taking seriously the warnings of the experts and the WHO. Without consulting the population, they are procuring hundreds of millions of packages of sparsely effective, expensive antiviral drugs and hundreds of millions of doses of hastily approved vaccines which are, after all, produced using conventional methods.
Critics, who describe the virus as comparatively harmless, are ridiculed or ignored initially. Finally, scientists, in Europe especially the German microbiologist and infection epidemiologist Prof. Sucharit Bhakdi, and the German pneumologist and politician Dr. Wolfgang Wodarg, gain media and political attention. The global madness, already threatening at that time, can be averted.
Worldwide, about 150 000 to 600 000 people died with or from H1N1, which turned out to be less dangerous than seasonal influenza. Correspondingly, vaccination readiness was low. Nevertheless, in Sweden alone, about 700 children contracted disabling narcolepsy, sleeping sickness, caused by hastily approved unnecessary and unsafe vaccines. In Switzerland alone, 1.8 million vaccine doses were sold abroad or given away, and 8.9 million were disposed of.
There was hardly any media coverage of the swine flu scandal. The temporary success of the media-fuelled panic was primarily due to the interconnectedness of experts, the pharmaceutical industry, the WHO and health politicians. In the end, the seemingly completely overwhelmed health authorities had fallen for an almost perfectly orchestrated propaganda campaign.
I recommend you watch the documentary ‘Profiteers of Fear – The Swine Flu Business’, produced in German by Arte in November 2009, and ask yourself: “Shouldn’t we all have learned a lot from this for the future?”

‘Event 201’: Corona Pandemic Simulation, 2019
The situation is threatening. A new corona virus is spreading across the world. Case numbers on the Johns Hopkins University dashboard are rising and rising. The highly contagious, immune-resistant, dangerous virus is paralysing trade and transport globally and sending the world economy into free fall.
What sounds like the alleged outbreak of the alleged pandemic of SARS-CoV-2 in China’s Wuhan province in December 2019, is the scenario of ‘Event 201’, which, because the figure zero is actually a globe, should rather be called “Event 21”.
On October 18th 2019, Bill and Melinda Gates Foundation, Johns Hopkins University and World Economic Forum are organising a pandemic simulation under this name. After the Spanish flu, the bird flu and the swine flu, they do not choose another influenza virus as the pathogen, but a corona virus that was completely unknown to laypeople so far, especially not to politicians and journalists.
This simulation of a corona pandemic that broke out in South America is not attended by doctors, but by Western representatives of the organisers, the UN, the WHO, governments, authorities and global corporations from the fields of high finance, pharmaceuticals, logistics, tourism and the media, as well as Dr George Gao, virologist and director of the Chinese Center for Disease Control and Prevention (CDC).

The participants agree that a corona pandemic is disruptive, can only be overcome by global governmental and private cooperation, that system-relevant global corporations must be propped up financially while medium-sized businesses must be sacrificed if necessary, that voices who deviate from the prevailing narrative must be censored consistently in the social and mass media, and that the pandemic can only be terminated by vaccinating the entire world population.
The simulation ends with 65 million deaths worldwide.
I recommend you watch the documentary ‘Event 201: Corona Pandemic from the Drafting Table’, produced in German with English subtitles by ExpressZeitung in June 2020, and ask yourself: “Shouldn’t the mass media have reported on this in detail?”
Corona Scandal, 2020 and ongoing
Two and a half months later, on December 31st 2019, the Chinese CDC, led by Dr. George Gao, reports 27 cases of pneumonia of unknown cause to the WHO – out of a Chinese population of 1.4 billion. On January 7th 2020, the Chinese health authorities identify a novel corona virus as the causative agent.
On January 21st, Prof. Christian Drosten et al. submit a paper, the recipe for which laboratories can produce a rapid RT-PCR test for the detection of the virus called ‘2019-nCoV’. It is accepted just the next day and published in the journal Eurosurveillance another day later.
The WHO had already posted the Corman-Drosten RT-PCR quick test on its website one week earlier and recommended it as the global diagnostic gold standard.
On January 30th, Drosten et al. published the justification of the narrative of epidemiologically relevant asymptomatic transmission of 2019-nCoV in the letter to the editor of the ‘New England Journal of Medicine’, virtually one of the bibles of us doctors whose integrity we still trusted at the time, with the title ‘Transmission of 2019-nCoV Infection from an Asymptomatic Contact in Germany’.
On February 11th, the WHO names the novel corona virus SARS-CoV-2, the disease it causes COVID-19; coronavirus disease. It does so against the request of Chinese virologists. They preferred to call it HCoV-19, human coronavirus, because of the danger that the name SARS-CoV-2 could stir up unfounded fears out of its biological and epidemiological lack of similarity to the much more dangerous SARS-CoV-1.
On March 11th, the WHO declares a COVID pandemic. Meanwhile, its Director-General, the biologist, immunologist and philosopher Dr. Tedros Adhanom Ghebreyesus, has been charged with genocide in Ethiopia before the International Criminal Court in The Hague. The presumption of innocence applies, of course.
Now, almost everything is going on as it did during the swine flu scandal in 2009, but in an even more lubricated way. Experts, mostly laboratory physicians and biologists working as virologists or epidemiologists, who have never examined anyone suffering from a respiratory infection, let alone treated them, declare that SARS-CoV-2 is virtually an alien about which we know absolutely nothing and that we must regard as extremely dangerous, until largely the same experts will have proven otherwise at some point. In Switzerland, they constitute themselves as ‘Swiss National COVID-19 Science Task Force’ and offer themselves to the Swiss Federal Council as scientific advisors.
The executive and legislative politicians as well as the federal and cantonal health authorities, all panicked by them, accept their offer and seem to follow them as blindly as the Federal Council apparently blindly followed the WHO when it declared the COVID pandemic. Unlike any ninepins club, the now official scientific advisory board to the Swiss government through what is supposed to be Switzerland’s biggest crisis since the Second World War does not keep any record of its activities.
On March 16th, the Swiss Federal Council declares the ‘exceptional situation’, the highest danger level of the epidemic law, based on exactly zero scientific evidence.
The mass media, including the Swiss public service broadcaster SRG, take on the third part in this conglomerate of mutually escalating ignorance, arrogance, incompetence and organised irresponsibility. Brainless and heartless themselves, they hammer into our heads around the clock:
There is a pandemic of a highly contagious and even epidemiologically relevant asymptomatically transmissible corona killer virus. Every seemingly hale and hearty fellow human being can be your angel of death!
Unlike in 2009, the mass media consistently censor, discredit and defame questioning doctors and scientists, including luminaries such as John Ioannidis, Professor of medicine, epidemiology and public health at Stanford University School of Medicine, one of the world’s most renowned and most cited scientists, specialised in science fraud, Prof. Sucharit Bhakdi, and Dr. Wolfgang Wodarg. At Easter 2020, after having been libelled, including an alleged threat to politicians and to my family, by a private person well known to me, myself, was brutally arrested by an anti-terrorist squad in my practice and, after it immediately turned out that I had not threatened anyone, merely the world view of insane people, I was shipped off to a closed psychiatric ward for six days because of ‘self-endangerment while in COVID insanity’.
The governments of almost all countries seem to have forgotten their epidemic plans, which wisely spare the individuals, the society and the economy. In blind obedience to the WHO and to lobbyists, called experts, they are enacting self-destructive non-pharmacological interventions, including lockdowns never considered before, following the authoritarian Chinese role model. They are doing this almost globally, in lockstep.
Without consulting the population, they procure billions of doses of emergency mRNA and DNA injections, which are even temporarily approved by Swissmedic. This technology is being widely used on humans for the first time. Almost worldwide, the constitution, the rule of law, human rights, civil liberties, ethics, science and common sense are being sacrificed in favour of a quasi-global authoritarian regime under the control of the WHO.
Who controls the WHO, controls the world!
The prevailing corona narrative is this: Since early 2020, there is a pandemic of a perennial killer virus, that must be searched for with the Corman-Drosten RT-PCR test in everybody, that is even spreading epidemiologically relevantly asymptomatically, against which there is no basic or cross-immunity, whose provoked disease, COVID-19, is barely treatable, which is becoming increasingly infectious and dangerous due to erratic mutations, and which can only be overcome by non-pharmacological measures that have never been applied before, such as antisocial distancing, masks in public sphere, contact tracing, isolation, quarantine, school closures and curfews, nowadays called lockdowns, even for asymptomatic, previously called healthy, people, and by serial vaccination of the entire world population.
All myths of the prevailing corona narrative are made up out of a fact-free vacuum
Based on the current state of science, these are my top 10.
1. There has been no epidemic of COVID-19 of national scope in any country, no pandemic internationally, for the general population SARS-CoV-2 is not a killer virus, and it is the same in every country. In many countries, for example in Switzerland, there was no exceptional excess mortality when adjusted to changing demographics. The excess mortality in other countries is the best proof that the real killer is not the virus, but our paradoxical response to it, which differs from country to country and from jurisdiction to jurisdiction. Also, the occupancy of the intensive care units, whose capacities have been massively reduced in the course of the alleged pandemic, has never been unusually high. If the causes of death are established correctly by substituting the number of deceased from whatever cause within 28 days after a positive RT-PCR test with the number of deceased from COVID-19, the infection fatality rate, IFR, is below that of influenza viruses, which are deadly to some people, of course, and, unlike SARS-CoV-2, sometimes are also deadly to children.
2. The indication to test, namely not only critically ill hospitalised patients with a need for specific antiviral therapy, in the surveillance system for respiratory infections and in an epidemiological study cohort, but to test even asymptomatic people and, on top of that, to test only for one single of all respiratory viruses that must be considered in the differential diagnosis of respiratory infections, is wrong.
3. The Corman-Drosten RT-PCR test is neither diagnostic for an infection with SARS-CoV-2 nor for a sickness or death from COVID-19. On November 27th 2020, an international group of 22 life scientists, including myself, published an ‘External Peer Review of the Corman-Drosten Paper’, the recipe by which laboratories developed the RT-PCR test for SARS-CoV-2. In it, we declared that conflicts of interest existed, that the alleged peer review within 24 hours was absurd, and ten fundamental scientific flaws. This most momentous medical publication of 2020, which can hardly be surpassed in terms of lack of scientificity, should never have been published. The Corman-Drosten RT-PCR test protocol is fabricated poorly and vaguely, without validation and standardisation. From a laboratory survey conducted in Germany, we know that due to cross-reaction with other beta coronaviruses its specificity of about 98.6%, corresponding to 1.4% false positives, which is already low in the absence of any virus, is further reduced to up to 92.4%, corresponding to 7.6% false positives, during the flu season. These rates of false positive tests may seem low to many laypeople and allegedly even to many ‘experts’, because they do not realise that in the virtual absence of the virus between the flu seasons, at prevalence close to 0, almost all positive RT-PCR tests are false positives. Please consider that if we test 1000 men with a 99% specific pregnancy test, 1%, 10 tests, will be positive and because of prevalence 0 of pregnancy in men, these positive pregnancy tests are all false positives. Everywhere, the test is performed differently and at too high cycle thresholds. Although studies have shown that no culturable viruses are present in samples with a Ct value above 28, the tests are still carried out with cycle threshold values above 35. Their results are reported without reference to clinical symptoms and findings, worldwide. The Corman-Drosten RT-PCR test is scientifically incorrect and serves mostly to create an epidemic of case numbers, a testing pandemic.
4. There is no epidemiologically relevant asymptomatic transmission of respiratory viruses. What we learned in medical school has been confirmed also for SARS-CoV-2 by numerous peer reviewed studies. The ‘asymptomatic contact’ invented by Prof. Drosten in the Letter to the Editor of January 30th 2020 was very much symptomatic: the patient had suppressed her symptoms with medication. Therefore, all non-pharmacological interventions for asymptomatic, formerly called healthy, people beyond the proven effective measures to contain the spread of respiratory viruses, namely hygiene and self-isolation of sick people, are harmful and ineffective also against SARS-CoV-2.
5. There is effective prophylaxis, for example, healthy lifestyle, lots of social contacts, and vitamin D3, and there is effective, well tolerated, low cost therapy of COVID-19, for example, anti-inflammatory drugs, topical budesonide, hydroxychloroquine, ivermectin, and anticoagulants.
6. Unlike influenza viruses, SARS-CoV-2 does not mutate erratically, but slowly and permanently. For this reason alone, even the most effective vaccines always lag behind its new variants.
7. SARS-CoV-2 is not becoming more and more contagious AND more and more dangerous. Like all other respiratory viruses, it obeys the laws of evolution. Without human intervention, the variant that spreads most easily prevails. That is why it is becoming more and more contagious indeed, but less and less dangerous, of course.
8. SARS-CoV-2, like all viral pathogens of acute respiratory infections, does not occur perennially, but seasonally, in our mid-northern latitudes from November to April.
What ‘experts’ call the heroic overcoming of the pandemic of a killer virus by non-pharmacological interventions and vaccination of the whole populace, we doctors call, the end of the flu season.
9. Due to basic and cross-immunity, during each flu season only about 10-20% of the population contract the seasonal beta corona and influenza viruses. This is also true for SARS-CoV-2.
An ‘nth wave of a respiratory virus’ is a biological impossibility.
Rather, the season of Corona-19 is followed by that of Corona-20 and now by that of Corona-21, to which most people are partially cross-immune, at least.
10. The alleged pandemic of the alleged killer virus SARS-CoV-2 cannot be overcome by vaccinating the entire world population, including the immune or recovered. The serial experimental mRNA and DNA injections are unnecessary because the IFR is 0.15%, for less than 70-year-olds below 0.05%, for children 0.00%, and even much lower if the causes of death are established correctly, so below that of seasonal influenza. Moreover, SARS-CoV-2 is mutating permanently and always in the sense that it becomes more infectious while less dangerous. The experimental foreign gene injections are ineffective. We had already known this from the registration studies, which are not worth the paper they are written on. For example, the mRNA injections reduced the risk of mild COVID-19 disease absolutely by less than 1%. There were no data for severe courses, for disease transmission and for over 75-year-old sick persons. Their ineffectiveness has also been proven in the real world by now. Finally, the gene injections are unsafe. They can cause anaphylactic reactions, thromboembolism, thrombocytopenia, disseminated intravascular coagulation, and myocarditis in the short term. There is possible immunosuppression and antibody-dependent enhancement, ADE, in the medium-term. And in the long term there are possible autoimmune diseases, cancer and infertility, risks that have not been ruled out yet. Furthermore, natural immunisation is stronger and more sustainable than the best vaccine, and immune or recovered people do neither need basic immunisation nor a booster. Or, if you had gone through measles, mumps and rubella as a child or had received the basic MMR immunization, did anyone ever recommend that you get vaccinated against measles, mumps and rubella for the first time or again? The mainly testing pandemic present since the end of the 2020 flu season, at least, can only be overcome by ending the unscientific testing of even asymptomatic people.
These are the major myths of the prevailing corona narrative. We doctors and scientists have not been allowed to debunk them publicly for over a year and a half. If we dare to fulfil our moral duty, we are ignored and censored at best, libelled, banned or forcibly detained psychiatrically, at worst.
Yet, in the second year, as medical students we had to study basic epidemiology. There we learned that in the event of a possible epidemic of national scope, a study cohort representative of the population must be formed immediately. Its purpose is to monitor the prevalence, incidence, and severity of the disease and the status of immunity, here by testing for antibodies AND T-cell immunity. Thus, in April 2020 we would already have realised that there was no epidemic of national scope, presumably that almost everyone was already largely immune and that there was exactly 0 scientific evidence for painful and costly nonsensical interventions, for the enactment of epidemic laws, for the drafting of COVID laws and for digital COVID certificates.
Allegedly, no one in the Swiss Federal Office of Public Health (FOPH) and in its affiliated Swiss National COVID-19 Science Task Force has the knowledge of a second-year medical student. For, although it is 20 months since the WHO declared the COVID pandemic, such a representative epidemiological surveillance cohort does not exist. Even worse, from week 13 to 44/2020 the FOPH had also paused the surveillance system of viral respiratory infections based on representative medical practices, thereby completing the blind flight in favour of total interpretive sovereignty of the arbitrarily manipulable useless RT-PCR test ‘case numbers’. Do not gloat. It is the same shame in your country.
It is wrong to test symptomatic people for only one of all respiratory viruses. It is insane to do this only with a hypersensitive, nonspecific RT-PCR test with cycle threshold above 35, without considering number of cycles, symptomatology and clinical context. It is even more insane to mass test also asymptomatic, previously called healthy, people in this way. And it is the coronation of insanity to serially administer unnecessary, ineffective, unsafe experimental mRNA and DNA injections to the entire world population, on top of that without regard to their immune status.
Should this text seem too long or too complicated to you, please take a close look at this picture. at least: It paints a thousand words.
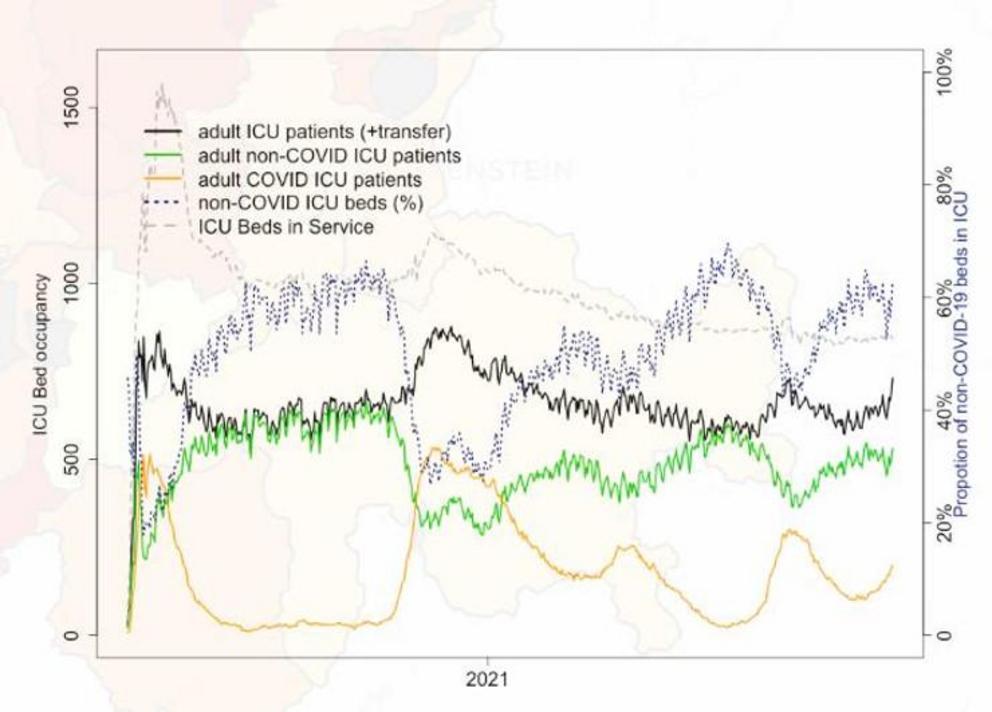
Just a glance at near-real-time monitoring of intensive care occupancy by ETH Zurich, state November 26th, 2021, exposes the fundamental fraud of the prevailing corona narrative.
During each alleged wave happens the same. Completely synchronously and to almost the same extent as the number of COVID patients, yellow curve, goes up, the number of non-COVID patients, green curve, goes down, although there are high reserves of intensive care beds, dashed curve, throughout the whole course of he alleged epidemic. At the end of each alleged wave, the same thing happens in the opposite directions.
Either, we believe that the very moment a COVID patient enters an intensive care unit a supernatural entity is postponing non-emergency major surgery, another viral pneumonia, a bacterial or fungal pneumonia, a myocardial infarction, a central pulmonary embolism, a cerebral stroke, or a major car accident with numerous serious injuries. Or, on admission to hospital every patient is tested for SARS-CoV-2 using the RT-PCR test, which is unsuitable for diagnostic purposes – rolling a dice would be cheaper. According to the test result, he or she is assigned to the green, non-COVID patients, or the yellow, COVID patients, curve, in short: other diagnoses are often mislabelled as COVID-19. This fraud occurs not so much in the intensive care units themselves, as rather in the direct reporting by the laboratories to the FOPH, which reports these and all other meaningless “case numbers” to the mass media, who then bombard us with them around the clock.
Since April 2020, at least, the total number of ICU patients, black curve, changes little due to this fundamental fraud in the prevailing corona narrative. It also explains why the intensive care units were not overloaded in any country, regardless of whether there are almost three times as many ICU beds per capita, for example in Germany, or only about half as many, for example in Sweden, as in Switzerland.
Those responsible must have known this. Otherwise they would not have cut ICU capacity worldwide since April 2020, in Switzerland from over 1500 to under 900, but would have built up more. Instead of redistributing 100 billion taxpayers’ Swiss Francs from the bottom and the middle to the very top, I would have recommended to my government investing a fraction of it in recruiting retired and in increasing the workload of part-time ICU staff.
I guess the coming so-called 5th wave will be very similar to the so-called 2nd wave during the last flu season with the usual hump in the total number of ICU patients, black curve, due to more frequent severe acute respiratory infections during every flu season.
I wish that the alleged ‘killer variant’ Omicron is natural and will therefore be more contagious, but less dangerous than the alleged ‘killer variant’ Delta, and that there will not be many very severe COVID cases due to ADE, and not too many very severe adverse events of the experimental mRNA and DNA injections.
Should you have a better explanation for the almost perfect symmetry of the yellow and green curves with an imaginary mirror axis located between the two, I will be the first to examine it closely and publicly apologize for my, then fake news.
SARS-CoV-2 is not an alien, but a newly discovered member of the well-known beta corona virus family. From my allegedly crazed cardiologist’s view, this is the prevailing corona nonsense narrative.
An endemic of a seasonal beta corona cold virus, that may kill some people, of course, and becomes increasingly harmless through permanent slow mutation, has been inflated into a pandemic of a perennial killer virus, which is becoming ever more dangerous through erratic mutations, with PR, PCR, frightening masks, and the myth of epidemiologically relevant asymptomatic transmission, that can only be overcome with pointless, harmful non-pharmacological interventions even for asymptomatic, formerly called healthy, people and with serial unnecessary, ineffective, unsafe experimental mRNA and DNA injections of the entire world population.
If you still do not realise that this is, pardon, utter nonsense, from A for epidemiologically relevant Asymptomatic transmission to Z for Zero COVID, I am afraid I can’t help you either and this German proverb comes to my mind, translated into English:
The greater the damage of the roof, the more beautiful the view of the stars!
The still prevailing corona nonsense narrative justifies the globally dominating unscientific, inhumane madness. Such can be wrought with any respiratory virus, by the way: if we no longer test everybody with a hypersensitive, low-specific RT-PCR test, that cross-reacts with other viruses, for theoretically one RNA fragment of SARS-CoV-2, but for one of, say, influenza or metapneumo viruses, we immediately have an influenza or metapneumo virus testing pandemic.
The alleged pandemic is mainly an unreal PCR testing pandemic, but the totalitarian repressive measures it has spawned are real: they threaten our freedom, our livelihoods and even our lives.
Dear responsible colleagues!
Please remember the Hippocratic Oath, ‘Primum non nocere, secundum cavere, tertium sanare’; ‘First do no harm, second be careful, third heal’, and the Geneva Declaration of the World Medical Association, especially ‘I will not use my medical knowledge to violate human rights and civil liberties, even under threat! Finally help to end this total insanity, first and foremost by no longer applying unnecessary, ineffective, unsafe experimental mRNA and DNA injections and by reporting all their adverse events. Then the corona house of nonsense cards will immediately collapse.
Dear responsible fellow Swiss!
Wake up, stand up and vote against the unscientific, unconstitutional, unlawful, inhumane, insane COVID law, for you, for your loved ones and for the whole human family, today!
Dear responsible fellow humans!
Wake up, stand up and fight, peacefully but firmly; if not for yourself, then for your children’s future and that of your grandchildren, now!